February 26th, 2025 | 15 min. read
You're finally ready to take the next big step on your IVF journey - egg retrieval and embryo creation. This is an exciting stage, but can also feel disheartening as you receive daily reports of your dwindling egg or embryo count. Is this normal? And what is the IVF attrition rate?
A fertility expert explaining the IVF attrition process to a couple.
Skip to a section:
- Growing Your Family Through IVF
- What is IVF attrition rate?
- Egg Development: Menstrual Cycle vs. IVF Cycle
- The 3 Phases of IVF Attrition
- Phase 1: Egg Retrieval
- Phase 2: Fertilization
- Phase 3: Embryo Growth & Development
- What percentage of fertilized eggs make it to blastocyst?
- What factors influence IVF attrition rates?
- Why don't all eggs create healthy embryos?
- What are my chances of pregnancy with IVF?
- Can IVF attrition be prevented?
- Can you assess egg quality before retrieval?
- How many blastocysts can be expected from 6 fertilized eggs?
- What is the embryo survival rate from Day 3 to Day 5 in IVF?
- What percentage of fertilized eggs survive and develop into embryos by Day 5?
- The Bottom Line: Attrition is Normal
Growing Your Family Through IVF
When you seek the help of a fertility specialist to conceive, you will undergo an array of diagnostic tests and have a comprehensive consultation with your new doctor before deciding on the best course of treatment together.
If the answer to your fertility challenge is in vitro fertilization (IVF) treatment, this next step comes with its own set of questions, such as "How long does the IVF process take?" and "What are the do's and don'ts during an IVF cycle?"
But the most common question we hear is usually, "How many embryos will I have at the end of this process?" To get to the answer, it's important to understand IVF attrition.
What is IVF attrition rate?
While you and your Care Team want the best outcome possible, it is important to have realistic expectations about the IVF process. One aspect of in vitro fertilization (IVF) that is essential to understand is called attrition.
IVF attrition is the rate at which your viable genetic material (eggs or embryos) taper off once they are in the embryology lab and growing.
In other words, the number of eggs that are retrieved are not likely to result in an equal amount of embryos. Instead, they will gradually decrease in number as they go from retrieved egg, to maturity, to fertilization, and then through the various stages of embryo development.
The bottom line? Not every egg retrieved will become a viable embryo. As hard as this can be to accept, try to remember that attrition is completely normal (and expected).
It may feel overwhelming to hear this, but remember - this is exactly how conception works in the natural process as well. With IVF, we just have the privilege of seeing this natural attrition happen in real time in the embryology laboratory.
Egg Development: Menstrual Cycle vs. IVF Cycle
It all starts with the egg!
In a typical menstrual cycle, several follicles (the fluid-filled sac that contains the egg) are created. One becomes dominant and the rest are reabsorbed back into the body. That dominant follicle releases an egg into the fallopian tube during ovulation and can then be fertilized by sperm.
In an IVF cycle, we manipulate that normal cycle with a special mix of medications that stimulate the ovaries to create as many dominant follicles as possible (instead of just one).
During this follicular stimulation phase, we try to maximize the number of viable eggs by "triggering" ovulation at the optimal time, when the highest number of eggs will be mature. The "trigger shot" is your final injection in an IVF cycle before retrieval.
Common medications to trigger ovulation include Novarel, Pregnyl, Ovidrel, and Lupron.
The 3 Phases of IVF Attrition
Let’s break the IVF attrition process down into three phases using concrete numbers so you can see how this might play out during an average fertility treatment cycle. By the end, you'll have a better understanding of why not all eggs retrieved will create viable embryos.

A visual representation of the IVF attrition process.
Phase 1: Egg Retrieval
When the follicular growth phase is complete (but before ovulation), we carefully remove each egg from its follicle through a minor surgical process called egg retrieval. During egg retrieval, eggs are collected from the ovaries so they can be fertilized with sperm in a laboratory.
Let’s say (for example) that your doctor collects 12 eggs during your egg retrieval. Unfortunately, not all 12 eggs will be viable (or useable). Why? Because only mature eggs will successfully fertilize.
While our goal is to retrieve only mature eggs, they naturally grow at different paces, leaving us with some variation in viability. During your egg retrieval, a team of embryologists will be carefully assessing each egg to determine maturity and viability.
Out of those 12 retrieved eggs, gathered at the peak of growth before ovulation, we expect that an average of approximately 80% will be mature. That leaves us with 10 viable eggs.
Visual learner? Watch this video to hear Nurse Monica explain this process further.
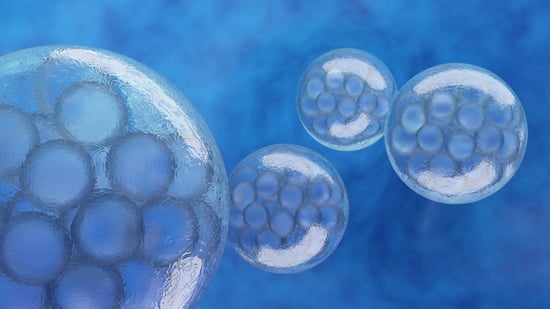
 Diagram showing the stages of embryo development from fertilization to blastocyst in IVF.
Diagram showing the stages of embryo development from fertilization to blastocyst in IVF.
Phase 2: Fertilization
The fertilization process has to happen naturally overnight with your partner's (or donor's) sperm in the IVF laboratory. This happens in one of two ways: conventional insemination or intracytoplasmic sperm injection (ICSI).
Both methods are very effective and may be used for different reasons:
- Conventional insemination is when the egg is surrounded by a deposit of sperm in a petri dish. Because one sperm will find its own way into the egg for fertilization, this mimics natural selection as best we can in a laboratory setting. There are multiple reasons to choose this method, one of which is good sperm quality.
- Intracytoplasmic sperm injection (ICSI) is when an embryologist selects a single sperm and manually injects it into the egg to fertilize it. ICSI is used for several different reasons, one being male factor infertility.
Either way, we expect that 80% of the mature eggs will fertilize. Now we have 8 fertilized eggs (referred to from here on out as embryos).
Phase 3: Embryo Growth & Development
The next big hurdle for these microscopic embryos will be continuing to develop in the IVF laboratory for the next 5-6 days. This is another phase where attrition should be expected. After 3 days, embryos have 6-8 cells. In general, most (if not all) embryos that fertilize will reach this stage.
The greatest attrition occurs between day 3 and day 5 or 6 (the blastocyst stage). A blastocyst is the final stage of embryo growth before we cryopreserve (freeze) them or perform an embryo transfer.
Only 30-50% of embryos growing on day 3 will reach the blastocyst stage. In this example, of those 8 embryos that originally fertilized, around 3-4 of them will be viable for transfer.
Note: If you're interested in getting your embryos tested prior to your transfer, a biopsy will be performed at this stage and the sample(s) will be sent off for in-depth preimplantation genetic testing (PGT) before cryopreserving (freezing) them.
Thinking about IVF?
Download our free guide to IVF to learn more about how much it costs, how long it typically takes, and how this fertility treatment can help you.

Your IVF Attrition Questions, Answered
Here are some of the most commonly asked questions about the in vitro fertilization (IVF) process, specifically pertaining to embryo development and IVF attrition:
What is the IVF attrition rate?
The IVF attrition rate refers to the percentage of fertilized eggs that do not progress to the blastocyst stage, with many embryos failing to survive or divide as expected.
What percentage of fertilized eggs make it to blastocyst?
On average, only 30-50% of fertilized eggs make it to the blastocyst stage.
While the percentage of fertilized eggs reaching the blastocyst stage may seem low, it's important to remember that the blastocyst stage represents a critical milestone in embryo development.
Embryos that reach this stage are generally considered healthier and have a higher chance of successful implantation and pregnancy.
What factors influence IVF attrition rates?
Attrition rates remain fairly steady, but can vary based on several factors, including:
- Female age: Younger women tend to have higher rates of blastocyst formation compared to older women. Age 35 is the typical point fertility begins to decline.
- Egg quality: High-quality eggs are more likely to develop into blastocysts.
- Embryo quality: Embryos with normal chromosomal makeup (i.e. those without too few or too many chromosomes) have a higher chance of reaching the blastocyst stage.
- Specific IVF cycle: Blastocyst formation rates can vary from cycle to cycle.
Why don't all eggs create healthy embryos?
This is a great question, with a somewhat unsatisfying answer:
Attrition is simply part of the natural selection process. The good news is that each phase of the attrition process reduces the likelihood of a non-viable embryo being transferred (which often results in the embryo not implanting successfully or leads to miscarriage, for example).
That being said, it can be hard to accept this process! You have every right to be frustrated or grieve the potential of your eggs and/or embryos that don't make it to the finish line.
We know how hard you've worked to get to this point, and hearing that those numbers are decreasing day by day can be incredibly disheartening.
Need extra support? Reach out to your nurse or navigator to schedule an appointment with a licensed fertility counselor who understands the unique challenges of treatment.
What are my chances of pregnancy with IVF?
In vitro fertilization (IVF) has come a long way since the first IVF baby was born in the UK in 1978. In women under the age of 37, the transfer of just one single blastocyst (embryo) offers a strong 50-55% chance of a healthy pregnancy!
In women over the age of 37, that percentage can be lower, but with advancements in embryo testing and the transfer of a chromosomally normal embryo, the chance of pregnancy still hovers around 50-55%.
Every situation is unique, and many factors can affect your outcome, but this does provide a general outline as to what to expect. Whether you’re in an opposite-sex relationship, looking to become a single mother by choice, or are an LGBTQ+ couple in need of a donor and IVF to have a baby, these numbers will still reflect the average rate of attrition.
Can IVF attrition be prevented?
Since IVF attrition is a natural decrease in the number of viable embryos during the IVF process, it cannot be completely prevented. However, there are steps that can be taken to minimize it and improve the chances of successful embryo development:
-
Comprehensive fertility assessment: A thorough evaluation of both partners' current fertility can help identify any underlying issues that might contribute to higher rates of attrition. This typically includes diagnostic testing to assess ovarian reserve, sperm quality, hormone levels, and genetic markers.
-
Personalized treatment: Tailoring IVF protocols to each patient's specific needs can optimize ovarian stimulation and egg retrieval, potentially improving embryo quality.
-
Advanced laboratory techniques: Utilizing state-of-the-art techniques like intracytoplasmic sperm injection (ICSI), assisted hatching, and preimplantation genetic testing (PGT) can help identify and select the healthiest embryos for transfer, potentially reducing the rate of attrition.
-
Optimal embryo culture conditions: Ensuring the best possible environment for embryo development in the laboratory, including temperature, pH, and nutrient levels, can enhance embryo survival and growth. This is why choosing a fertility clinic that is CLIA and CAP accredited is so important.
IUI & IVF Success Rates
Wondering what your personal chances of success with fertility treatment might be? Dr. Ilana Ressler breaks down IUI and IVF success rates by age in this helpful guide.

Can you assess egg quality before retrieval?
There is no foolproof way to assess egg quality definitively before undergoing retrieval, but certain biological factors and tests can provide some insights, such as:
Maternal Age
A woman's age is the most significant factor influencing egg quality. As women age, the percentage of chromosomally normal eggs decreases, leading to a higher risk of miscarriage and genetic abnormalities in embryos.
Hormone Tests
- Anti-Mullerian Hormone (AMH): This hormone is produced by the cells surrounding the eggs in the ovaries. AMH levels can indicate the size of the remaining egg pool and provide an estimate of ovarian reserve.
- Follicle-Stimulating Hormone (FSH): This hormone is responsible for stimulating the growth of eggs in the ovaries. Elevated FSH levels, especially on day 3 of the menstrual cycle, can suggest diminished ovarian reserve.
- Estradiol: This hormone is produced by the growing follicles. High estradiol levels during ovarian stimulation can indicate a good response and potentially a higher number of eggs retrieved.
Basal Antral Follicle Count
During a transvaginal ultrasound, your provider can count the number of follicles in the ovaries during the early follicular phase of the menstrual cycle. A higher follicle count can be associated with a better response to ovarian stimulation and a higher number of eggs retrieved - though this is not always true.
Understanding the Limitations
- These tests provide indirect measures of egg quality and don't guarantee the presence of healthy, mature eggs capable of fertilization and normal embryo development.
- The only way to definitively assess egg quality is to fertilize the eggs and evaluate the resulting embryos for chromosomal abnormalities.
While these tests can offer valuable information about potential egg quality and ovarian reserve, they should be interpreted with caution and in conjunction with other factors like age and medical history.
Discussing your individual situation with a fertility specialist is crucial to make informed decisions about your treatment options.
How many blastocysts can be expected from 6 fertilized eggs?
Typically, about 2 to 3 of the 6 fertilized eggs may develop into blastocysts, though this can vary depending on individual factors like egg quality and embryology practices.
What is the embryo survival rate from Day 3 to Day 5 in IVF?
The survival rate from Day 3 to Day 5 can be between 30% to 50%, depending on the quality of the embryos and the laboratory conditions.
What percentage of fertilized eggs survive and develop into embryos by Day 5?
Around 40% to 50% of fertilized eggs survive and develop into embryos by Day 5, with some embryos failing to progress beyond earlier stages.
The Bottom Line: Attrition is Normal
While IVF attrition may be a difficult concept to grapple with, the most important thing to know is that this process is natural and expected, regardless of your diagnosis.
Remember: Even one embryo at the end of an IVF cycle offers you an excellent chance at a healthy pregnancy, and the sooner you begin your fertility treatment journey, the better your chances are of getting more high-quality embryos.
If you're struggling to conceive and want to explore potential pathways to parenthood, the team at Illume Fertility is here to help make your dreams come true. When you're ready to take the next step, reach out to us to get started.
Is IVF right for me?
Take our fertility quiz and get personalized recommendations on treatment pathways.
